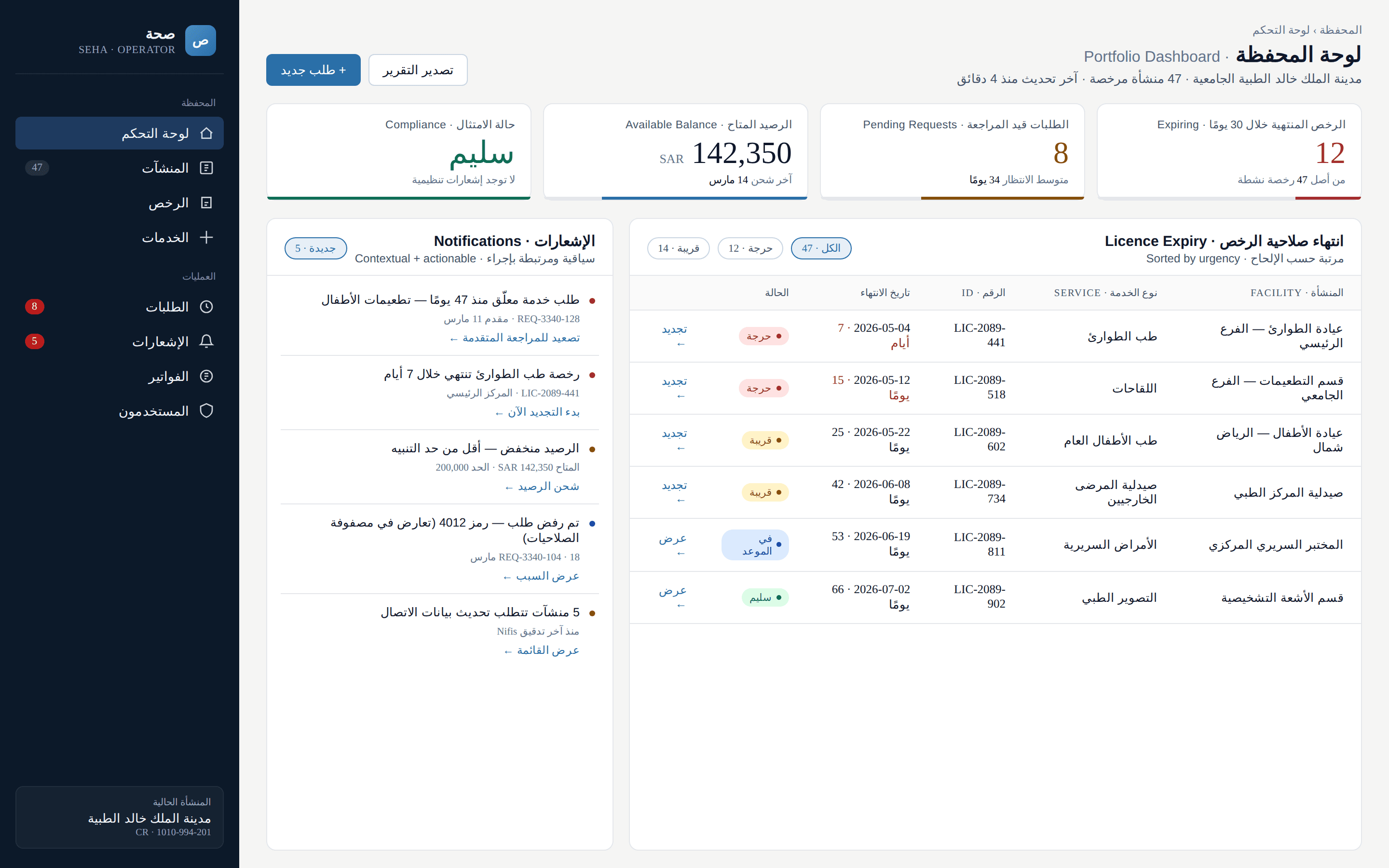
the platform was built around the licensing process — not the people running hospitals.
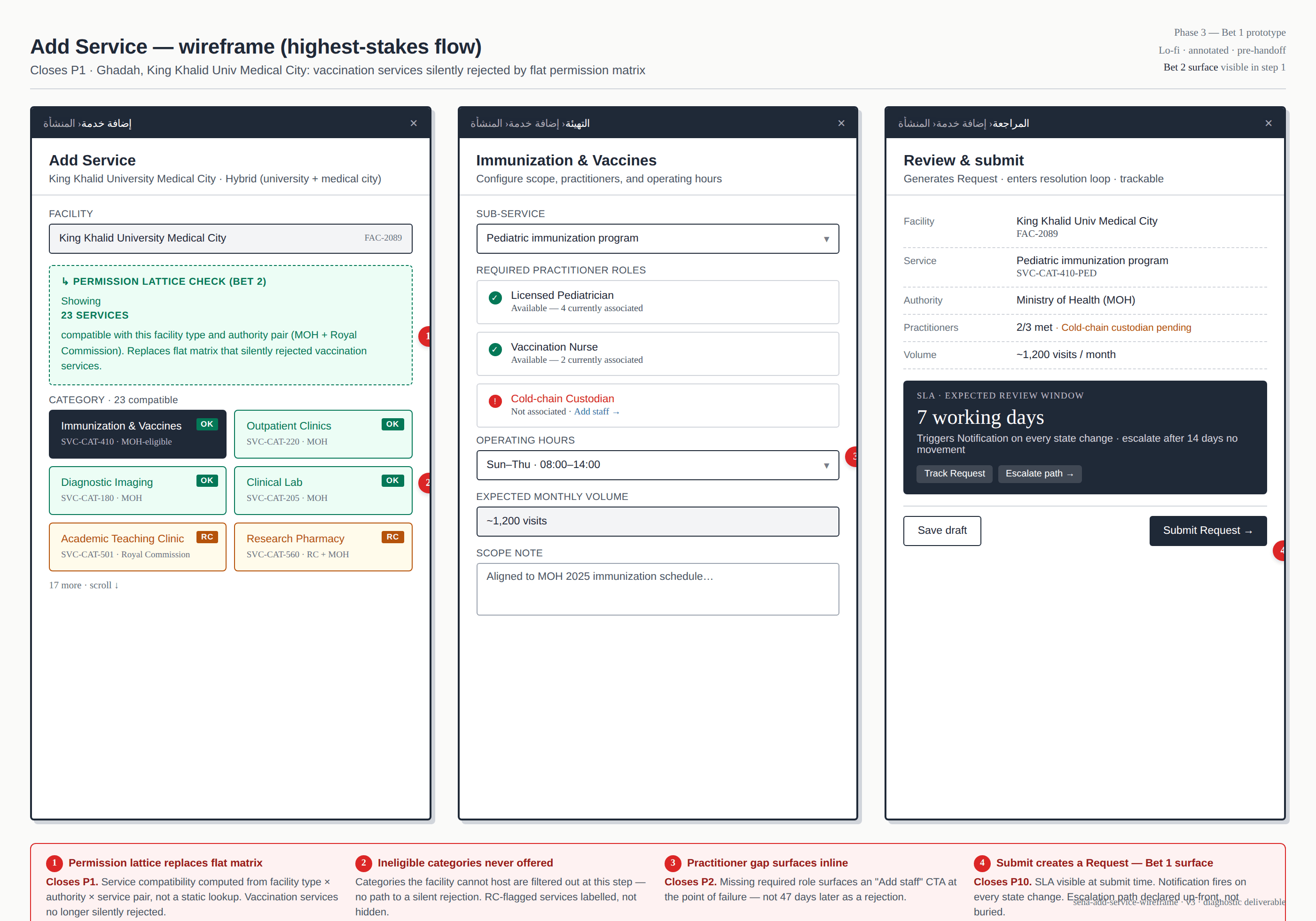
Saudi institutional operators — university medical cities, hospital networks, hybrid academic-clinical institutions — depend on Seha to add services, staff, and facility types as their operations evolve. By the time the diagnostic began, those operators were stuck. Service requests sat for two months and longer with no status update. Permission matrices silently rejected legitimate combinations: a medical city could not add vaccination services because the facility type and the service type were incompatible in the underlying model. Operators couldn't add new medical staff because their roles didn't exist in the permission system at all. The platform's scope had outgrown its information model — and the cost was operational paralysis at the institutions Saudi healthcare depends on most.