the platform was built around an engineering achievement — not around the clinicians using it.
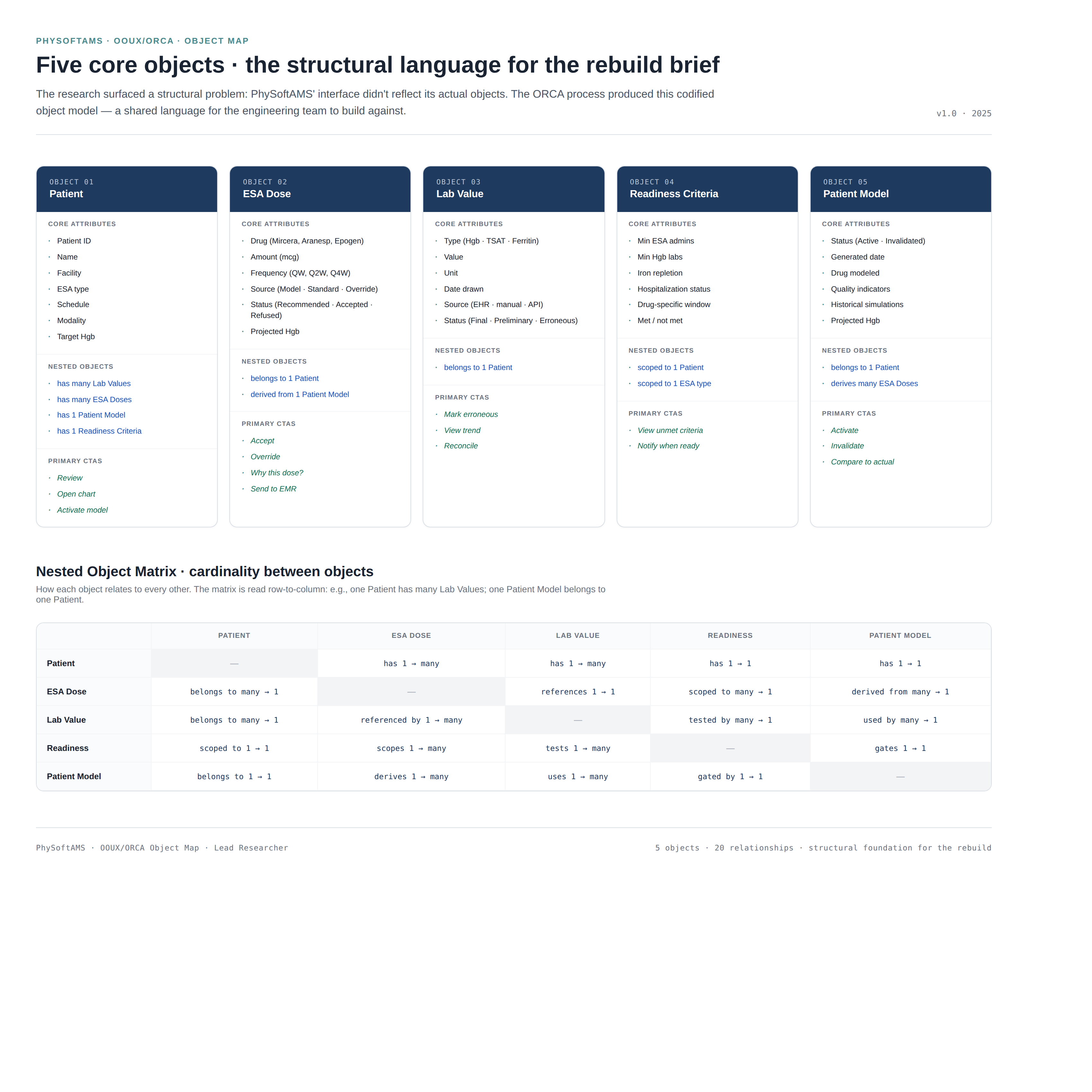
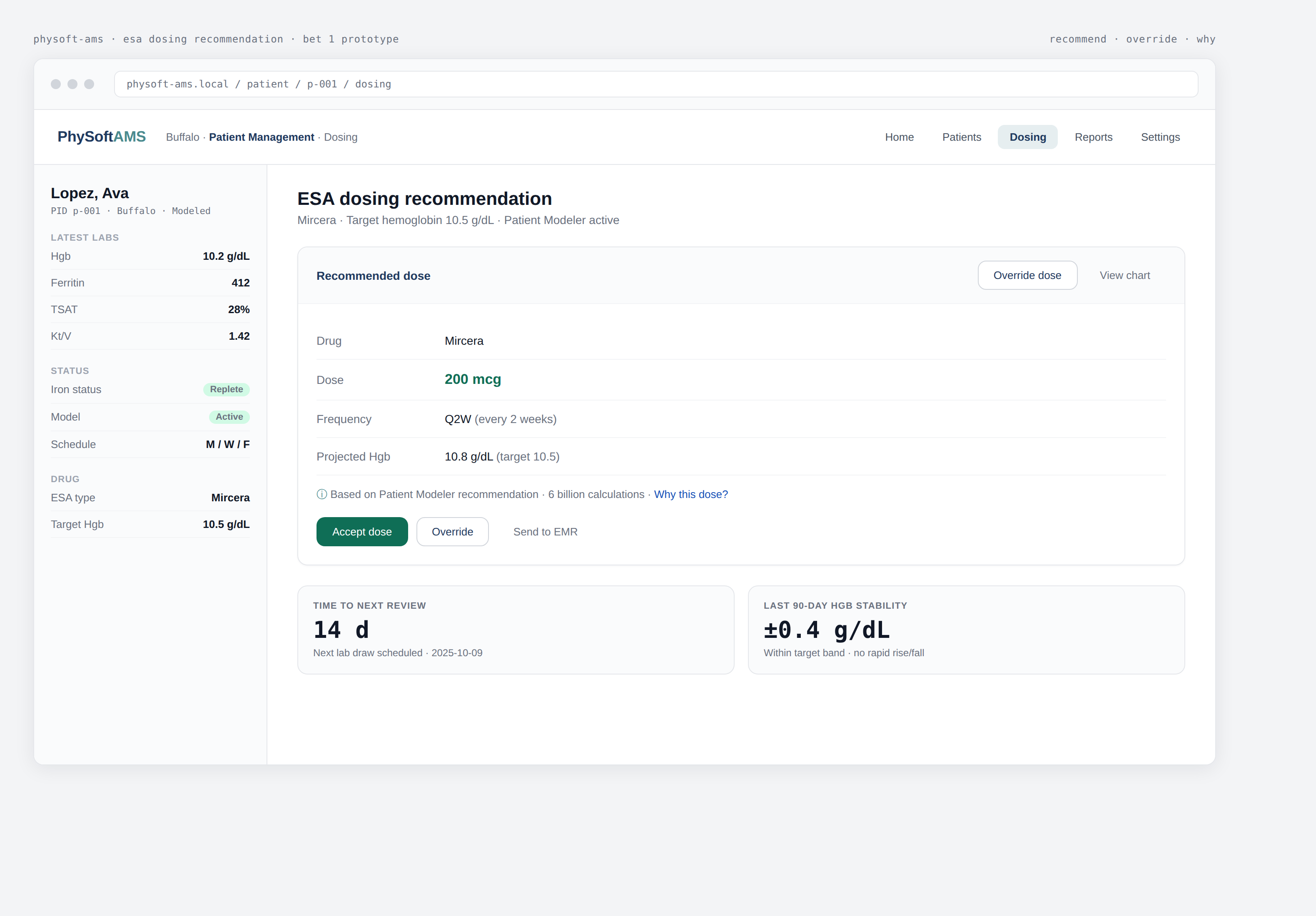
PhySoftAMS contains a genuinely sophisticated PK/PD engine. The Patient Modeler runs roughly 6 billion calculations per patient to produce individualized ESA dosing recommendations — the kind of precision that is supposed to make narrow-therapeutic-index drug management safer and cheaper. The Expert System fills the gap when patients do not have enough data to model. On paper, this is best-in-class clinical decision support.
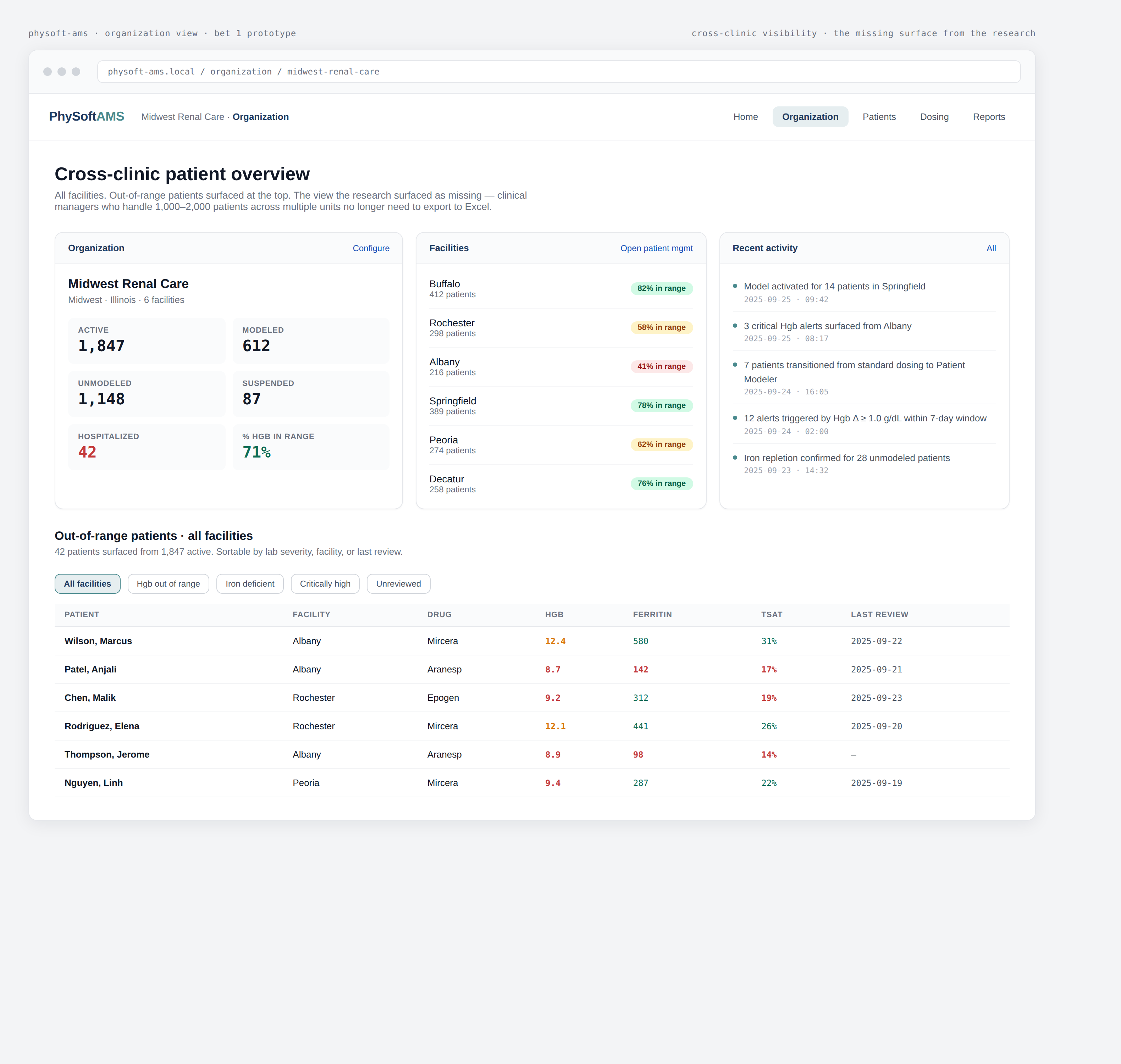
But the research surfaced a quieter truth. The platform had been designed around the algorithm, not the people who use it. Experienced nurses arrive with a paper tracker already filled in. They review labs in another tool before they ever log in. The system is not where decisions get made — it is where decisions get documented after the fact. Adoption was strongest among the system's own designers and a small group of power users; everyone else was working around it.